

*** This article was updated on 28 July to include a statement from Australia’s Chief Medical Officer.
Alison Barrett writes:
Australia should implement a coordinated response to stop transmission of monkeypox and protect priority populations in response to the recent World Health Organization declaration of monkeypox as a Public Health Emergency of International Concern (PHEIC).
The WHO declaration also means that countries like Australia should intensify public health measures such as supports for isolating infected individuals, contact tracing, vaccination, and targeted use of pre-exposure prophylaxis vaccinations in high-exposure populations.
As well, countries like Australia that have reported cases of monkeypox within the last 21 days should strengthen clinical management and infection prevention and control in healthcare settings and hasten research on the use of vaccines, therapeutics and other tools, according to the declaration.
Croakey was unable to find a statement from the Australian Government Department of Health website regarding the WHO’s determination of monkeypox as a PHEIC. We asked the DOH to provide a comment, but no response was received as of late on 27 July.
Public health emergency
The WHO declared monkeypox to be a PHEIC after a second meeting of the International Health Regulations (IHR) (2005) Emergency Committee regarding the outbreak on 23 July.
According to the WHO, the Committee were not able to reach consensus regarding their advice to declare monkeypox as a PHEIC; WHO Director-General Tedros Adhanom Ghebreyesus made the final decision.
Under the IHR, a Public Health Emergency of International Concern is
an extraordinary event, which constitutes a public health risk to other States through international spread, and which potentially requires a coordinated international response.”
Committee Members’ views in support of a determination of PHEIC included:
- That the outbreak of monkeypox meets the three criteria for PHEIC
- Rising trends in global cases and countries where monkeypox is reported
- Cases reported in children and pregnant women
- Support and resources required for the LGBTIQA+ community, who are the most affected community affected outside Africa
- Modes of transmission in current outbreak not fully understood
- Perceived benefits of declaring it a PHEIC include maintaining awareness, boosting international coordinated and political commitments to response.
The views of Committee Members not in support of PHEIC:
- The overall global risk assessment has not changed since 23 June 2022
- Based on available data, no indications of exponential increase in the number of cases
- Most cases are observed among men who have sex with men with multiple partners and there was a perception that there is still opportunity to stop ongoing transmission with targeted interventions in this group
- Perceived low severity of the disease.
Ghebreyesus said:
Although I am declaring a public health emergency of international concern, for the moment this is an outbreak that is concentrated among men who have sex with men, especially those with multiple sexual partners.
That means that this is an outbreak that can be stopped with the right strategies in the right groups.
It’s therefore essential that all countries work closely with communities of men who have sex with men, to design and deliver effective information and services, and to adopt measures that protect the health, human rights and dignity of affected communities.
Stigma and discrimination can be as dangerous as any virus.”
Global health expert Professor Kathryn H. Jacobsen wrote in The Conversation that the declaration was not a cause for panic, but “it is a way to prevent monkeypox from becoming a global crisis”.
Recommendations
Temporary recommendations for countries’ response to the monkeypox outbreak were also issued by the WHO at the IHR meeting.
Based on epidemiological situation, patterns of transmission and capacities, different recommendations apply to different countries.
“All temporary recommendations are expected to be implemented in full respect of established principles of human rights, inclusion and the dignity of all individuals and communities,” says the WHO.
Recommendations for four identified groups of countries follow:
1. Those that have no history of monkeypox in human populations or have not detected a case for over 21 days.
The main recommendation is to strengthen “all aspects of readiness for responding to monkeypox and stop human to human transmission”, including disease surveillance and identification, testing, raising awareness and risk communication among current high-risk groups.
2. Those with recently imported cases of monkeypox in human population and are experiencing human-to-human transmission.
The main recommendations are to “implement a coordinated response to stop transmission” and protect priority populations.
Intensify public health measures such as supports for isolating infected individuals, contact tracing, vaccination, and targeted use of pre-exposure prophylaxis vaccinations in high-exposure populations (such as healthcare workers)
To strengthen clinical management and infection prevention and control in healthcare settings and hasten research on the use of vaccines, therapeutics and other tools.
3. Those with transmission of monkeypox between animals and humans.
Recommended to undertake detailed case studies of transmission between animals and humans to gain a better understanding of transmission patterns.
4. Countries with manufacturing capacity for vaccines, diagnostics and therapeutics should increase production and work with WHO to ensure they are distributed “at reasonable cost to countries where they are most needed to support efforts to stop the onward spread of monkeypox”.
Full recommendations can be viewed in this statement.
Concerns were raised at the meeting about the pricing and distribution of vaccines and antivirals and the need to ensure they were available equitably.
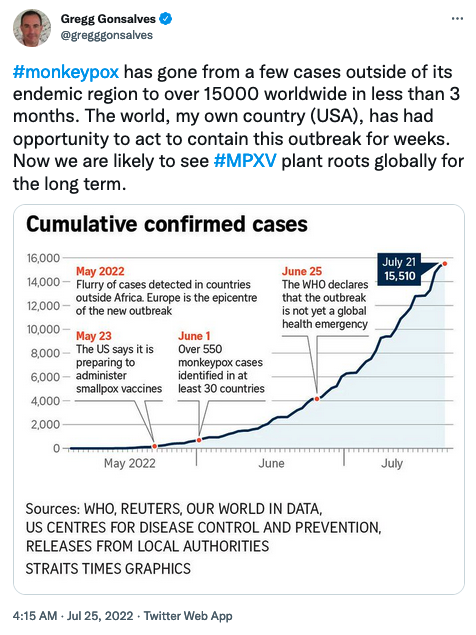
As suggested by the tweets below, the decision raises questions and concerns about the potential for discrimination, stigma and human rights abuses.
Australia’s response
As Australia has reported cases of monkeypox within the last 21 days, that would have us sit under Group Two of recommendations, with a need to intensify public health measures and implement a coordinated response to stop transmission.
Associate Professor Michael Burke, a GP in Western Sydney, told newsGP that “general practitioners have a very key role to play, they need to be aware of the symptomatology, then do the appropriate testing and ensure that people do the necessary isolation,” he said.
Last week, Croakey reported that the Federal Government has been urged to vaccinate at risk groups and that containment of the virus “would be best achieved with antiviral treatments and third generation smallpox vaccines”.
The determination of monkeypox as a PHEIC, along with COVID-19 and polio, and future emerging infectious diseases has been linked to plans for an Australian Centre for Disease Prevention and Control, as tweeted by Public Health Association of Australia president Dr Tarun Weeramanthri. He called for national communications to inform the public about the significance of the WHO declaration..

More from Twitter




Follow this list of monkeypox sources.
Update on 28 July
Australia’s Chief Medical Officer, Professor Paul Kelly, released a statement declaring monkeypox a Communicable Disease Incident of National Significance.
“This follows the World Health Organization (WHO) declaring the global situation regarding MPX to be a public health emergency of international concern,” Kelly said in the statement.
View the full statement here.
The Australian Technical Advisory Group on Immunisation (ATAGI) has updated its guidance on vaccination against monkeypox.
Please see Croakey’s archive of articles on monkeypox.







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}