

“It should be recognised that for victims who have suffered for years and have not received any or very little adequate help, that help may be required for the rest of our lives as behaviour and coping mechanisms have become entrenched over the many years since the sexual abuse.” Survivor testimony.
The Final Report of the Royal Commission into Institutional Responses to Child Sexual Abuse, handed down late last year, contains important reading – as well as calls to action and to account – for health and social services and systems as well as the disability and aged care sectors.
It includes a range of recommendations for sectors and services providing therapeutic treatments or other services to victims and survivors as part of an overall call for integrated systems, evidence-based trauma-informed policy and practice, and a life course approach.
The recommendations range from the creation a national centre for children and adults who experienced sexual abuse in childhood (to make sure the “momentum” of the Royal Commission does not stall and to fill vital gaps in research and knowledge translation around trauma and therapeutic care) to a call for Primary Health Networks to support sexual assault services to work collaboratively with other key services across sectors.
The Royal Commission raises particular concerns for abuse victims and survivors with disability, emerging from out-of-home care or within the justice system, living in rural or regional areas, and entering aged care, particularly for members of the Stolen Generations, Forgotten Australians and Former Child Migrants – an issue also raised last year in the Bringing Them Home 20 years on report.
 With a focus on the impact of abuse and the protective role of culture that has been welcomed by the Secretariat of National Aboriginal and Islander Child Care (SNAICC) and the Australian Indigenous Doctors Association (AIDA) (see tweet, right), it calls for Aboriginal and Torres Strait Islander healing approaches to be an “ongoing, integral part of advocacy and support and therapeutic treatment service system responses”.
With a focus on the impact of abuse and the protective role of culture that has been welcomed by the Secretariat of National Aboriginal and Islander Child Care (SNAICC) and the Australian Indigenous Doctors Association (AIDA) (see tweet, right), it calls for Aboriginal and Torres Strait Islander healing approaches to be an “ongoing, integral part of advocacy and support and therapeutic treatment service system responses”.
Its overall message to service systems is that:
“Inadequate service responses can re-traumatise survivors of child sexual abuse. Poor therapeutic treatment can leave a victim with chronic symptoms that follow them into adulthood. Ineffective treatment may cause victims to lose hope and disengage from treatment altogether.”
The need to do no more harm
 The Royal Commission’s Final Report generated huge media coverage when it was delivered to the Governor-General and publicly released on 15 December 2017, after holding 57 public hearings and more than 8,000 private sessions over five years.
The Royal Commission’s Final Report generated huge media coverage when it was delivered to the Governor-General and publicly released on 15 December 2017, after holding 57 public hearings and more than 8,000 private sessions over five years.
Yet those stories have barely been able to touch the surface of the report which comprises 17 volumes and includes 189 new recommendations, on top of the 409 from other reports already released on Criminal Justice, Redress and Civil Litigation and Working With Children Checks.
Many of the recommendations are to do with making institutions safer for children, but others are focused on trying to ensure that effective support – and no further harm – comes to victims and survivors through systems that are supposed to support them.
Volume 9, Advocacy, support and therapeutic treatment services looks at what the Royal Commission learned about survivors’ needs in terms of advocacy, support and treatment from a range of services: mental health, alcohol and other drug, community health, GPs and psychologists, Aboriginal community controlled health services, disability services, aged care, and specialist services, such as child and adult sexual assault services.
It offers nine recommendations (listed below) for improving service systems to better respond to survivors’ needs (beyond those already accepted by the Federal Government as redress responses, such as psychological counselling)
“Their needs have long been left unmet”
Volume 9 says the Royal Commission heard many examples of services assisting victims and survivors to heal but that child sexual abuse is still a taboo subject for many of the public and for professionals, and “remains misunderstood, under-reported, under-identified and under-treated”.
It says quality standards for the delivery of advocacy and support and therapeutic treatment services are inconsistent, services are often “piecemeal”, and limited skills and expertise in working with child sexual abuse and trauma – along with gaps in affordable services – compound service issues for victims and survivors.
It refers to a consensus statement issued to it last year by the mental health commissions of Australia, describing the mental health service system as ‘highly siloed’, where services (and funding) are often driven by diagnosis or presenting behaviours and with clearly demarcated outcomes.
“The system rarely works strategically and collaboratively to privilege an individual’s holistic recovery across the life cycle,” the statement said.
At the practitioner level, the Royal Commission says that a lack of understanding about child sexual abuse can lead to disclosures being “denied, dismissed or downplayed”. At the policy level, it says that despite being over-represented in several service settings, survivors are not recognised in key national policy frameworks: “as a result, their needs have long been left unmet”.
It quotes New South Wales Mental Health Commissioner John Feneley on why that matters:
“I have to say, I have a great faith in primary care and general practice, but you need to find the time and to help them prioritise the need for their practices to become trauma-informed. Again, there are some great models out there where entire practices rebuild their services around recovery focused trauma-informed care principles, where everybody from the receptionist through to the doctor has this firmly in mind. But that won’t happen overnight. So we need to have policy settings that encourage it and reward it to make sure that it happens.”
Multiple systems and services over many years
The report talks in detail about the “profound, long-lasting and cumulative impacts” that the trauma of institutional child sexual abuse can have on victims and survivors who, at various times, depending on the circumstances, seek support from a range of mainstream and specialist services to help manage the detrimental impacts of abuse on their mental health.
It raises one survivor’s story of the various services she had used to manage the impacts of child sexual abuse she had experienced as a ward of the state. These included legal services, out-of-home care support services, practical support from a service for Forgotten Australians, psychiatric support, in-home peer support, alcohol and other drug treatment services, a therapeutic community she stayed in as a resident and victim support groups.
However, it reports that services span sectors and can be difficult to navigate, including for secondary victims, such as family members and carers. It said:
“Currently, service systems across Australia do not have the capacity to meet victims’ and survivors’ needs. Inadequacies are most apparent when a victim or survivor is experiencing multiple and complex impacts from the trauma of child sexual abuse, particularly for those deemed as not fitting within the remit of a single service. In many cases, one individual will be in multiple systems, moving in and out of services over many years.”
In the 218 page volume, the Royal Commission details the strong messages it heard from victims and survivors about the barriers they faced when seeking help from services.
“Many survivors said they faced stigmatising community and professional attitudes about child sexual abuse. We were told that information was difficult to find and that services were often prohibitively expensive. We also heard about the range of systemic and structural barriers that created difficulties for survivors. This included the fragmentation of the various service systems they access, the limited capacity of services to collaborate with one another, the lack of relevant knowledge among mainstream service providers, the scarcity of resources in specialist sectors and a lack of cultural competence and disability awareness.”
Digging down into “detrimental practices in front-line services”, it heard that agencies and professionals were often unaware of good practice for supporting victims and survivors, and often emphasised problems with the victim rather than with the perpetrators or acts of abuse. Some professionals specifically chose not to ask a client about possible childhood sexual abuse as they did not know how to respond, it said.
“Research into this issue suggests a range of reasons why clinicians in certain settings do not ask about histories of abuse, including: not wanting to be intrusive or inappropriate; not identifying a connection between the presenting problems and child sexual abuse; a belief that there were more immediate needs; a lack of time and resources; a fear of vicarious traumatisation; a concern about causing distress to clients; and a fear of inducing ‘false memories’.
But as well as warning of the impact of inadequate services on victims and survivors, including the risk of retraumatisation, the report says there is a cost to the community in poor use of public funding and also for those working the system themselves:
“For services and professionals, failing to improve collaboration can mean knowledge and skills remain compartmentalised. A workforce without the right skills, knowledge and support mechanisms not only diminishes the quality of service provision, but also puts at risk the wellbeing of professionals working in a challenging field. “
The Royal Commission also highlights gaps in research on the experiences and outcomes of survivors of institutional child sexual abuse, and in “limited” evidence on the effectiveness of therapeutic treatment. It said:
“In particular, research to better understand therapeutic treatment approaches for a range of specific groups is needed. Currently, the coordination and translation of knowledge about trauma-informed approaches into practice is ad hoc, impacting workforce skills and exacerbating shortages in expertise.”
Summary of recommendations
Recommendation 9.1
The Australian Government and state and territory governments should fund dedicated community support services for victims and survivors in each jurisdiction, to provide an integrated model of advocacy and support and counselling to children and adults who experienced childhood sexual abuse in institutional contexts.
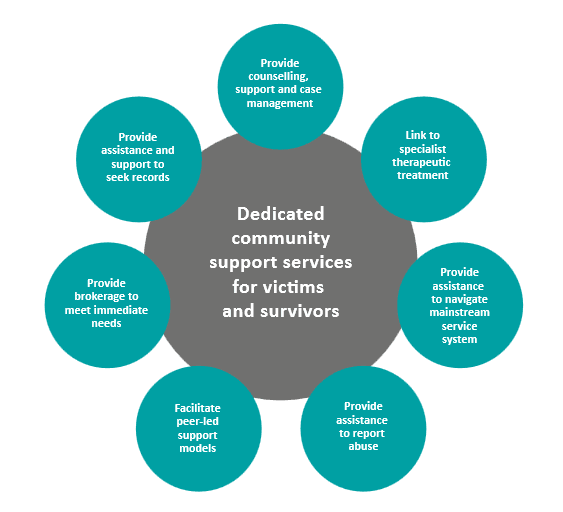 Funding and related agreements should require and enable these services to:
Funding and related agreements should require and enable these services to:
- be trauma-informed and have an understanding of institutional child sexual abuse
- be collaborative, available, accessible, acceptable and high quality
- use case management and brokerage to coordinate and meet service needs
- support and supervise peer-led support models.
Recommendation 9.2
The Australian Government and state and territory governments should fund Aboriginal and Torres Strait Islander healing approaches as an ongoing, integral part of advocacy and support and therapeutic treatment service system responses for victims and survivors of child sexual abuse. It recommends that these approaches be evaluated in accordance with culturally appropriate methodologies, to contribute to evidence of best practice.
Recommendation 9.3
The Australian Government and state and territory governments should fund support services for people with disability who have experienced sexual abuse in childhood as an ongoing, integral part of advocacy and support and therapeutic treatment service system responses for victims and survivors of child sexual abuse.
Recommendation 9.4
The Australian Government should establish and fund a legal advice and referral service for victims and survivors of institutional child sexual abuse, including to provide advice about accessing, amending and annotating records from institutions, and options for initiating police, civil litigation or redress processes as required.
Recommendation 9.5
The Australian Government should fund a national website and helpline as a gateway to accessible advice and information on childhood sexual abuse, to provide information for victims and survivors, but also to the general public and practitioners about supporting children and adults who have experienced sexual abuse in childhood and available services.
Recommendation 9.6
The Australian Government and state and territory governments should address existing specialist sexual assault service gaps by increasing funding for adult and child sexual assault services in each jurisdiction, to provide advocacy and support and specialist therapeutic treatment for victims and survivors, particularly victims and survivors of institutional child sexual abuse.
Funding agreements should require and enable services to:
- be trauma-informed and have an understanding of institutional child sexual abuse
- be collaborative, available, accessible, acceptable and high quality
- use collaborative community development approaches
- provide staff with supervision and professional development.
Recommendation 9.7
Primary Health Networks, within their role to commission joined up local primary care services, should support sexual assault services to work collaboratively with key services such as disability-specific services, Aboriginal and Torres Strait Islander services, culturally and linguistically diverse services, youth justice, aged care and child and youth services to better meet the needs of victims and survivors.
Recommendation 9.8
The Australian Government and state and territory government agencies responsible for the delivery of human services should ensure relevant policy frameworks and strategies recognise the needs of victims and survivors and the benefits of implementing trauma-informed approaches.
Recommendation 9.9
The Australian Government, in conjunction with state and territory governments, should establish and fund a national centre to raise awareness and understanding of the impacts of child sexual abuse, support help-seeking and guide best practice advocacy and support and therapeutic treatment, and lead a national research agenda.
It says the centre’s activities should:
- identify, translate and promote research in easily available and accessible formats for advocacy and support and therapeutic treatment practitioners
- produce national training materials and best practice clinical resources
- partner with training organisations to conduct training and workforce development programs
- influence national tertiary curricula to incorporate child sexual abuse and trauma-informed care
- inform government policy making
It says the national centre should partner with survivors in all its work, valuing their knowledge and experience.








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}